Guide to Tumor lysis syndrome: Vital things to know
Guide to Tumor lysis syndrome: Vital things to know
- onco
- October 3, 2020
Guide to Tumor lysis syndrome: Vital things to know
What is tumor lysis syndrome?
Tumor lysis syndrome ( TLS ) refers to the condition of metabolic disturbance which occurs when a large number of tumor cells or neoplastic cells are killed briskly within a short period, leading to the release of intracellular components in the blood. This syndrome is characterized by the quick development of hyperkalemia, hyperuricemia, hyperphosphatemia, hypocalcemia, with acute kidney injury and is hazardous.
TLS is common in people having blood-related cancer and lymphoma( lymphatic cancer). It initially rises through chemotherapy. Risk factors include tumors with rapid cell growth and movement, hematologic cancers like acute leukemia, or tumors with a high sensitivity to chemotherapy.
Patients with high levels of lactate dehydrogenase (greater than 1,000 U/L) and people with damaged renal function are also at risk. Various chemotherapy agents like cisplatin, etoposide, cytarabine, and paclitaxel are also connected with this syndrome.
How does it develop?
Not all cancer patients have an equal rate of developing this syndrome. TLS is most likely to happen when blood disorders and cancer are treated with chemotherapy. In highly reproducing cancer acute leukemia, few cells die before the treatment as it’s the end of their life cycle.
If a huge amount of these cells lyse and die, TLS may grow before the beginning of the treatment. However, a huge amount of intracellular substances are released in the bloodstream as most of the neoplastic cells in the bone marrow and bloodstream of patients suffering from acute leukemia are destroyed through chemotherapy.
These cells get destroyed and die, a large amount of phosphate and potassium are released including purine nucleic acids.
Patients with huge “tumor burdens” (number of cancer cells in the body) or have rapidly dividing cells that respond well with treatment are at high risk. These include:
- Leukaemia
- Non-Hodgkin lymphoma
- Tumors like hepatoblastoma and neuroblastoma
- Myeloproliferative diseases or neoplasm
- Cancer that causes the ill function of the kidney before the treatment start
Other risks
- Intrathecal chemotherapy ( injection of chemotherapy, given directly into the fluid-filled space around the brain and spinal cord).
- Chemoembolization ( soothing treatment for tumors found in the liver).
- Radiation therapy (uses a beam of huge and intense energy to kill cancer cells)
- Corticosteroid therapy
- Hormonal and biological therapy
TLS usually develops within a few hours to 2-3 days after the start of the chemotherapy. The mortality rate of patients suffering from tumor lysis syndrome is less the 20%
What are the symptoms?
The symptoms of these syndromes may be lenient at first, but become hazardous over time due to the mixing of several substances in your systemic circulation. Symptoms of TLS include:
- Nausea, vomiting
- Weakness and fatigue
- Numbness, seizure, and tingling
- Muscle cramping and joint pain
- Hallucinations and confusion
- Decreased, dark urine
If TLS left untreated, it eventually leads to severe outcomes, these include:
- Seizures
- Abnormal heart rate
- Loss of muscle control
- Even death
Hyperkalemia, Hyperphosphatemia, Hypocalcemia and hyperuricemia
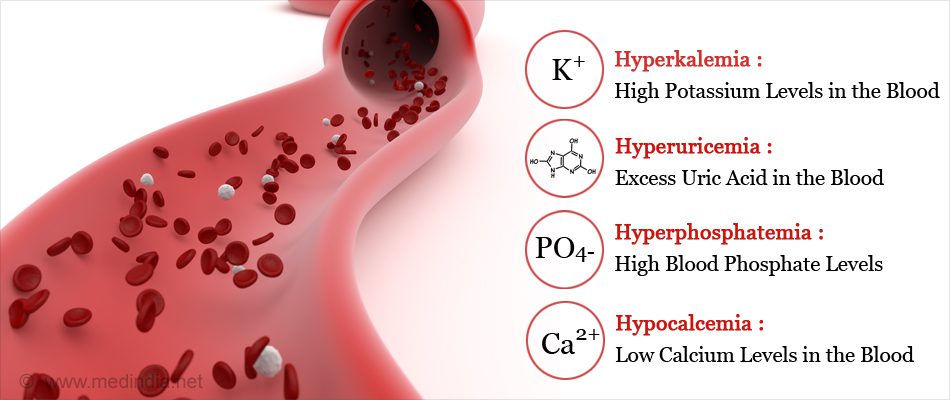
Generally, the first sign of TLS is hyperkalemia and the most dangerous component of this syndrome as potassium tends to leave the cell before they rupture. Hyperkalemia is defined as a medical condition of the body when it has too much potassium in the blood. Potassium is an important nutrient and helps in building nerves, muscles, and the heart.
Mild hyperkalemia is usually asymptomatic but chronic ones can cause a threat to life, cardiac arrhythmias, muscle weakness, or paralysis. This electrolyte can cause lethal dysrhythmias and damage normal cardiac functions. The kidneys aren’t able to excrete enough potassium to remunerate for the hyperkalemia as it is submerged by excess potassium.
Hyperphosphatemia is known as having a high level of phosphate in the blood released from the cancerous cells, phosphate is an electrolyte i.e. electrically charged substance that has phosphorus in it. The kidneys try to get rid of the excess amount of phosphorus in the bloodstream by increasing urine output and decreasing the amount of phosphorus reabsorption, but in the end, it reaches its limits where they can no longer payback, and phosphorus piles up in the blood. Generally, Hyperphosphatemia develops 1-2 days after the treatment.
As phosphate levels increase, phosphate ions (negatively charged) merge with calcium ions (positively charged) eventually leading to decreased serum calcium level. A condition where the body has really less than enough calcium is known as Hypocalcemia. It is also a sign of TLS. These calcium-phosphate complexes cause tubular obstruction and acute renal damage.
Neoplastic cells also release purine nucleic acid. Usually, purines are metabolized to hypoxanthine, converted to xanthine, and then to uric acid by the enzyme xanthine. An excess amount of purines are released rapidly in the blood during this syndrome. The kidneys are unable to excrete the overwhelming amount and results in hyperuricemia and uric acid formation in the kidneys. Hyperuricemia is seen 48 to 72 hours after the beginning of chemotherapy.
Due to these circumstances, the kidneys are submerged by excess phosphorus, potassium, uric acid crystals, and calcium phosphate precipitate leading to acute renal failure. The kidney tries to compensate for the increased electrolyte and uric acid by increasing the urine output, but can’t, due to uric acid nephropathy and volume depletion.
Lab work is carried out every 6 hours for the first 24 hours after chemotherapy started if a patient is in danger due to tumor lysis syndrome.
Diagnosis
Clinical signs, lab tests, and symptoms are used in diagnosing the tumor lysis syndrome.
The Cairo-bishop grading system, used in classifying and grading TLS, states lab anomalies in serum uric acid, phosphorus, potassium levels 25% increased over baseline, and serum calcium levels were decreased by 25% from baseline.
This system contemplates lab value alters that occur in patients from 3 days before to 7 days after the beginning of chemotherapy. The lab irregularity organized by the system is categorized based on cardiac dysrhythmias, seizures, severity including age-adjusted serum creatinine.
Tumor lysis syndrome is generally diagnosed by:
- Complete blood cell count
- Phosphorus and calcium test
- Urinalysis
- The uric acid level in the blood
- Creatinine level
Quick identification key
One can recover from this life-threatening problem of cancer treatment if they are promptly able to recognize the signs and symptoms of tumor lysis syndrome and take preventive measures.
Prevention and treatment of TLS
To help prevent TLS, the following steps you should be taken:
- Before the beginning of treatment, your healthcare will determine whether you have the risk of developing this syndrome. This is based on the type of cancer.
- Lab tests, checking conditions like poor kidney function, heart disease, or hypertension
- Medications like Allopurinol ( Lopurin, Zyloprim (Aloprim) should be taken, to reduce or stop the amount of uric acid and rasburicase (Elitek, Fasturtec) for breaking down the uric acid.
- The level of electrolyte should be balanced
- Level of calcium and potassium
Allopurinol
It stops the conversion of xanthine to uric acid and hypoxanthine to xanthine by inhibiting xanthine oxidase. Ideally, it starts 1-2 days before the starting of chemotherapy.
Monitors patients for any fever, allergies, or skin rash including nausea, vomiting, and chills. Common unfavorable results from the intake of allopurinol headache and drowsiness.
Allopurinol therapy is done before chemotherapy as it helps to prevent excess uric acid. It has no effect on patients suffering from hyperuricemia and it increases the level of xanthine that could damage the kidney.
It is never operated with capecitabine because allopurinol may deteriorate its effectiveness.
Rasburicase
Rasburicase is a drug that cures hyperuricemia, changes uric acid to allantoin. allantoin is more soluble than uric acid in urine. This drug decreases the level of uric acid and manages the amount of serum potassium, calcium, phosphate, and creatinine.
Also, it works quickly and takes 4-5 hours to show effectiveness. Patients should be well hydrated before taking this drug. Patients with large tumor burdens tend to take longer therapy (up to seven days or twice/day) while for other patients it is effective in 1-2 days.
Pay attention to the patient taking rasburicase while sending lab specimens for the uric acid level test. To maintain approx uric results, the blood samples must be kept on ice after being taken. Poorly ensured samples will give false results because any uric acid of the sample being reduced by rasburicase at room temperature.
Patients receiving this drug should not be supplied with allopurinol as it can interfere in the work of rasburicase and may decrease its effectiveness. Rasburicase should never be given to patients suffering from glucose-6-phosphate dehydrogenase deficiency due to the risk of critical hemolysis.
Stop giving this drug to the patient if it shows a sign of hypersensitivity. Signs of hypersensitivity reactions include bronchospasm, urticaria, dyspnea, chest discomfort, hypoxia, and hypotension. The most common unfavorable reactions of patients related to one dose of this drug infusion are headache, vomiting, and fever. But eventually results in urticaria pruritus, dyspnea, increased liver enzymes, and chest and back pain with increased or repeated dosing.
Healing the complications of TLS
- Patients with TLS should be provided with enough water and stay well hydrated before the treatments.
- IV calcium should not be delivered to patients with hyperphosphatemia, because it increases calcium phosphate precipitation.
- Hyperphosphatemia control is managed with phosphate binders such as aluminum hydroxide given in limited dosages to avoid aluminum toxicity. Other phosphate binders having calcium, such as calcium carbonate or calcium acetate may be used instead.
- Ensuring the sign and symptoms of hypomagnesemia from sodium sulfonate and hypocalcemia using sorbitol also the patient’s 12-lead ECG should also be monitored and maintained as it plays a role in indicating and accessing cardiac rate and rhythm for dysrhythmias.
- Patients having symptomatic hyperkalemia should be accessed with iv regular insulin and dextrose for redistributing potassium, within the cell.
- Patients not responding to these measures should be accessed to a renal replacement, such as hemodialysis, to manage renal failure and electrolyte anomalies.
Quick identification key
One can recover from this life-threatening problem of cancer treatment if they are promptly able to recognize the signs and symptoms of tumor lysis syndrome and take preventive measures.
Cautious of these medications!
A list of medication, patients suffering from TLS must avoid or there would worsen the effects of this syndrome:
- Acetylsalicylic acid,(aspirin)
- Medication containing potassium and phosphorus
- Beta-blockers
- Mannitol
- Some antibiotics
- Heparin
- Bisphosphonates
- Potassium-sparing diuretics
- Nephrotoxic agents such as aminoglycosides and nonsteroidal anti-inflammatory drugs
Book an appointment with the Best Cancer Specialist at Oncoplus Hospital.
Recent Posts
-

How to Prepare Yourself for Chemotherapy: Essential Tips and Guidance
November 19, 2024
-
Lung Cancer: Signs, Diagnosis, and Treatment Options
November 5, 2024
-
Tomotherapy where precision and efficiency meet health
October 28, 2024
-
What to Eat During Cancer Treatment: Nutrition Tips for Recovery
October 21, 2024
-
Best Blood Cancer Treatment in Delhi
October 8, 2024

Leave a Reply