The new standard of care for acute myeloid leukaemia

The new standard of care for acute myeloid leukaemia
- onco
- October 18, 2020
Myeloid Leukaemia (AML) is a rare but intense type of cancer of myeloid cells (white blood cells responsible for strengthening our immune system and fighting infection). The new standard of care for acute myeloid leukaemia is being tested all around the world for effective treatment of its patients.
The latest results from the VIALE-A phase III clinical trial from this summer revealed a 34% decrease in the death risk, by cementing a drug combination that’s been tested around the work. Phase III was a large multicenter clinical trial that was created to establish whether the combination of “Venetoclax ” and “azacitidine” is superior to azacitidine alone. It was a confirmatory study for the patients diagnosed with AML that we’re unable to tolerate intensive chemotherapy.
As Courtney DiNardo, MD, MSCE, Clinical Researcher in the Department of Leukaemia explained that most of the patients with AML are over the age of 65, which is an age where standard chemotherapies are not an ideal option. It has an increasing rate of toxicity and proves less effective. The main intentions of the phases III VIALE-A trail were to have better overall survival (OS) rate. Fortunately, the study was successful in showcasing it.
The response rate was 66% high, which explained that the majority of the people responded better with the regimen of “venetoclax” and “azacitidine”. The overall survival rate improved significantly in patients that have taken this combination. Even the timing of the response, people who studied and went into remission were excessively higher.
The majority of people who received venetoclax and azacitidine together achieved a diminution of severity of AML within the first cycle of the treatment. Or it was several months faster than the prior existing standard of care.
The new medication is completely different and live-changing in the treatment of cancer, especially AML. It’s the first confirmatory, phase II study that’s evident in showing something better from the previous standard of care, from azacitidine or a low dose of chemotherapy. The new treatment has proved that the drug combination has upgraded the outcomes in both remission rates and OS.
What makes this approach of treatment better than the rest?
There’s been numerous research and study done over the past few decades to improve the outcomes of people with AML. And various other treatments have tried treating the disease but the result has been elusive. AML has remained to be the most common kind of leukaemia in the world with a 5-year survival rate of 28%.
The combination of venetoclax, a first-in-class medicine added with azacitidine showed a great deal of improvement in older patients with AML. Backed with intensive research evidence and real-time effectiveness, this approach suggested being a potent drug combination.
What’s Venetoclax and Azacitidine?
Venetoclax is effective in treating adults with chronic lymphocytic leukaemia or small lymphocytic lymphoma. This medication targets the B-cell lymphoma-2 (BCL-2) protein that prevents some blood cancer cells from dying naturally from the process of apoptosis. It selectively binds to the BCL-2 protein and hinders it from coming in contact with cancer cells, which helps to restore apoptosis.
While Azacitidine is a chemotherapy drug that functions by allowing the bone marrow to grow normal blood cells, decrease the requirement for blood transfusions and kill abnormal blood cells. It’s placed in a class of medications, known as demethylating agents that are designed to target aberrations of DNA methylation patterns linked with cancer onset and progression.
How was VIALE-A clinical trial done?

In the double-blind, placebo-controlled, phase III VIALE-A clinical trial, about 433 people who haven’t received any treatment beforehand with AML and ineligible for intensive chemotherapy were randomized to take either a combination of venetoclax (n=286) arm or azacitidine in combination with a placebo arm (n=145).
The final results expected were primarily the overall survival (OS) rate and complete remission rate along with incomplete hematologic recovery in the United States, China, Japan, the European Union, and EU countries. While the secondary results were complete remission (CR) and CR with partial hematologic recovery (CR + CRH).
According to the researchers, people assigned with venetoclax and azacitidine arm combination in the VIALE-A trial have a median survival rate of 14.7 months against 9.6 months for people with the placebo arm.
Moreover, about 66.4% of people who received venetoclax plus azacitidine achieved CR+CRi against 28.3% for the azacitidine plus placebo group.
The safety of the procedure was mostly consistent among the patients with previous studies of venetoclax and azacitidine combination. The most adverse complication of the combined medication was the following:
-
- Hematologic and gastrointestinal nature (40%)
- Thrombocytopenia (46%)
- Nausea (44%)
- Constipation (43%)
- Diarrhea (41%)
- Febrile Neutropenia (42%)
- Neutropenia (42%)
The most common and severe reactions happened with less than 10% of patients given venetoclax and azacitidine are febrile neutropenia (30%) and pneumonia (17%).
Tumour lysis syndrome (TLS) was recognized during ramp-up in three patients in the venetoclax arm, but none in the placebo arm. As we all know, TLS is a severe complication of venetoclax due to the fast breakdown of cancer cells, often causing kidney failure, death, dialysis, and death.
Complications caused in the trial, however, were temporary, biochemical changes resolved with uricosuric agents and calcium supplements without treatment interruption.
What are the complications of the venetoclax + azacitidine regimen?
The biggest problem associated with the venetoclax and azacitidine regimen is its toxicity. It’s quite concerning according to the researchers. There’s already more myelosuppression due to lower white blood cell count due to this regimen. If you have neutropenia and neutropenia-related fever, then you must inform your doctors or physicians. But the toxicity is possible to be reduced at its lowest by the physicians.
The management of patients is the key importance when given the combination of the medication. Historically, patience with azacitidine alone didn’t go into remission until the fourth or sixth cycle of therapy. So researchers didn’t do routinely early bone marrows and required no major interventions and kept the patients on cycle due to their low blood counts when they still had leukaemia.
The combination, however, is different as the vast majority of patients go into remission within the first cycle, meaning it’s important to do bone marrow in the first cycle itself. Older patients with AML often have multiple medical conditions at the same time so physicians have to modify the treatment regimen down. Instead of the standard 4 weeks, physicians spread the 21-day regimen over 5 weeks. Doctors have to stop the therapy in between and wait for a week or two for counts to recover, then modify the treatment accordingly.
Monitoring guidelines are developed as a part of the study and available to help the physicians with the management of AML patients acquiring the venetoclax and azacitidine regimen. This drug combination is an incredibly effective regimen that’s well-tolerable if the patients are appropriately managed.
What’s to look for in AML cure?
The drug has turned into becoming standard care for older patients with AML, all over the USA. The FDA has also approved the regimen use in 2018, after the phase, I study that gave impressive response rates and the possibility of improvements to overall survival (OS).
After racing the phase III VIALE-A study, the results of the drug combination, this newfound regimen has rapidly adopted the standards of care across the world. There’s still a clinical implication, not just in US citizens but globally. But, this regimen is seen as a practice-changing new therapy globally where the complications can be reduced.
This regime is still an improved standard of care that’s not the same as eliminating the disease. We still need additional research for a new standard of care for AML. This regimen is not helpful for the majority of patients with AML.
Future research sources on the identity of patients with AML that aren’t likely to respond with the combination of venetoclax and azacitidine regimen. Hopefully, it works on people with certain gene mutations that have proved to respond poorly to the regimen.
In the care of TP53 mutations (TP53 is a gene that helps to cease the tumor growth. It acts and is known as a tumor suppressor), effective TP52-treatment to azacitidine and venetoclax that responds safely is still being worked upon.
Book an appointment with the Best Cancer Specialist at Oncoplus Hospital.
Recent Posts
-

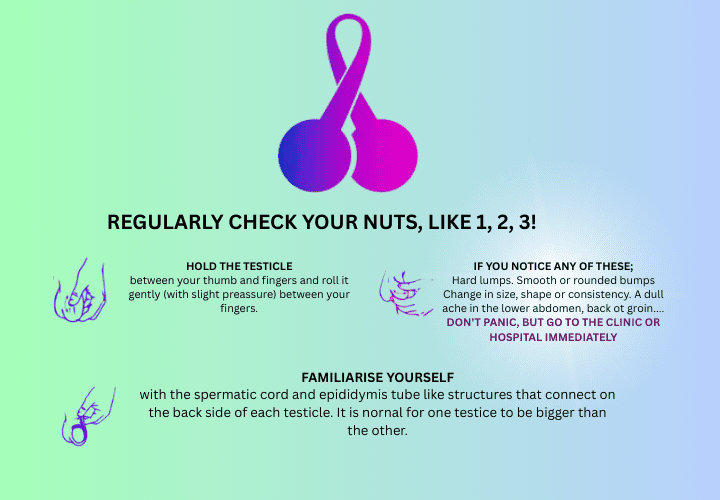
Can Testicular Cancer affect fertility?
April 23, 2025
-
Why are Breast Cancer Cases Increasing Around the World?
April 17, 2025

Leave a Reply